

Downloads
Download



This work is licensed under a Creative Commons Attribution 4.0 International License.
Article
Association between Cardiopulmonary Exercise Test and Severity of Obstructive Sleep Apnea Syndrome
Jianyu Wang 1,2, Sisi Zhang 2, Luying Jiang 3, Chunran Zhang 3, and Houjuan Zuo 2,*
1 Tianyou Hospital, Wuhan University of Science and Technology, Wuhan 430064, China
2 Division of Cardiology, Department of Internal Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, China
3 The 3rd Department of Cardiology, The First Affiliated Hospital of The Medical College, Shihezi University, Shihezi 832008, China
* Correspondence: zuohoujuan@163.com
Received: 17 April 2023
Accepted: 6 June 2023
Published: 27 December 2023
Abstract: Obstructive sleep apnea syndrome (OSAS) is becoming widespread, especially in people with obesity. As it is usually measured by polysomnography (PSG), the role of cardiopulmonary exercise test (CPET), a new exercise capacity test, has not attracted enough attention in OSAS research. In this article, we explore the relationship between CPET results and patients with OSAS. 68 individuals were recruited and divided into three groups: negative/mild group (n = 22, apnea hypopnea index (AHI) < 15), moderate group (n = 22, 15 ≤ AHI < 30) and severe group (n = 24, AHI ≥ 30). Clinical parameters, cardiopulmonary exercise test (CPET) indexes, and apnea hypopnea index (AHI) were compared among the three groups. A multivariate analysis was carried out to assess which factors determine the index of AHI. The ANOVA analyses were used to evaluate the difference among the three groups. Receiver operating characteristic analyses were chosen to detect the prediction efficiency of the CPET index for AHI. The predictive power of using the CPET index (VO2/kg peak) combined with the body mass index (BMI) of patients in the detection of AHI was significantly better when compared with using the CPET index only. There was a notable correlation between VO2 and the index of AHI (r = 0.249, P = 0.04). Also, the CPET data (VO2/kg peak) combined with the BMI of patients has powerful predictive value for the severity of OSAS in patients. It is expected to be a promising way to predict the severity of OSAS in the future. Our study provides a new strategy for predicting whether a patient is in the early phase OSAS.
Keywords:
cardiopulmonary exercise test (CPET) polysomnography obstructive sleep apnea syndrome (OSAS) prediction body mass index1. Introduction
Patients with obstructive sleep apnea syndrome (OSAS) are characterized by repeated collapse of the upper respiratory tract, which leads to sleep fragmentation and nocturnal hypoxemia [1]. OSAS is manifested as reduced night sleep, snoring, daytime sleepiness, and fatigue. It has been reported to be correlated with pulmonary hypertension, stroke, heart failure and metabolic diseases [2]. Increasingly, evidence shows that obesity is strongly correlated with OSAS [3]. Patients with moderate and severe OSAS often have an increased risk of developing a variety of diseases compared with unaffected individuals [4]. The diagnosis of OSAS in patients should encourage treatment with continuous positive airway pressure (CPAP) [5]. According to a clinical trial, oropharyngeal exercises significantly reduce OSAS severity and symptoms and represent a promising treatment for OSAS [6]. The drugs most commonly described as possible treatments for OSAS include progestogens, theophyllines and antidepressants. Previous studies have shown that SGLT-2 can significantly improve the symptoms of obstructive sleep apnea patients with obesity [7], but the effect needs further study. Formerly, polysomnography (PSG) was considered the gold standard for diagnosing sleep-related respiratory disorders, including OSAS and other sleep-related disorder diseases. In previous studies, the diagnosis and evaluation criteria of OSAS were apnea hypopnea index (AHI) and minimum oxygen saturation (LsaO2). AHI reflected the number of apnea times during night sleep, while the minimum oxygen saturation reflected the most serious hypoxic event [8]. Patients usually need plenty of time to complete this test, which made it difficult to know whether the patients had OSAS.
Cardiopulmonary exercise test (CPET), also known as the oxygen consumption test, is also a stress-loading test that measures the exercise capacity of the test subject. This technique is widely used in clinical practice to evaluate the causes of dyspnea and fatigue in patients; it can accurately distinguish between cardiovascular diseases, lung diseases and diseases of the locomotor system. It can optimize decision-making, predict results, guide subsequent treatment and evaluate therapeutic effects [9]. Nowadays, it is widely used in clinical practice when patients are suffering from symptoms, such as chest pain, shortness of breath, and leg fatigue during exercise [10]. By measuring the maximum oxygen uptake, the cardiopulmonary exercise experiments can determine the maximum exercise capacity of the participants. Peak VO2 values have a critical role in oxygen uptake and ventilatory patterns obtained during the submaximal portion of CPET. Peak VO2 is also valuable due to its ease of ascertainment during low-level exercise, its relevance to the ability to perform activities of daily living, and it is independent from volitional effort [11]. Despite an increasing scientific interest in OSAS in recent years, very little data investigating the predictive power of CPET combined with BMI in patients with OSAS is currently available. Our work aims to provide evidence for the potential utility of CPET in the clinical diagnosis of patients with OSAS. In this study, patients with different degrees of sleep apnea were included to explore the relationship between the CEPT index and the condition of patients with sleep apnea, and whether the CPET index can be used to predict the severity of patients with sleep apnea.
2. Methods and Materials
2.1. Population and Recruitment
In this study, we recruited 97 patients, including 68 male individuals and 29 female individuals at Tongji Hospital. All participants underwent overnight polysomnography (PSG) and were recruited after signing an institutional ethics committee-approved consent form. The average apnea and hypopnea per hour of sleep were defined as the apnea-hypopnea index (AHI), which was measured by a standard polysomnography system. The study focused on male participants because the analytic results (Supplemental data) of all 97 participants had no statistical significance, and most of the OSAS patients were male. The patients were divided into three groups according to AHI score: negative/mild group (AHI < 15, n = 22), moderate group (15 ≤ AHI < 30, n = 22), and severe group (AHI ≥ 30, n = 24). Because all baselines of the diseases were identical, there were no exclusion criteria. The demographic characteristics and laboratory evaluation included routine blood tests and electrocardiogram. Each patient signed the informed consent form.
2.2. Acquisition of Participants’ Characteristics
Height and body weight were measured, respectively, and the BMI was also calculated. Resting systolic and diastolic blood pressure and heartbeat were measured in the supine position. The arterial blood sample for the analysis was drawn with the patient in a sitting position on the day after the polygraphy registration and within one hour of waking up. Then the samples were frozen and stored at –80 ℃ until analysis. Blood parameters for basic characterization include total cholesterol, low- and high-density lipoproteins, and triglycerides.
2.3. Polysomnography (PSG)
Polysomnography (PSG) is a basic diagnostic tool used to assess sleep disorders. It also records sleep stages, eye movements, EMG tension, respiratory parameters, and an electrocardiogram. In particular, it is useful in measuring sleep-disordered breathing and its management; excessive sleepiness tendencies; and complex behaviors during sleep, including sleep movement disorders, sleep-related seizures, and hypersomnia. The diagnosis of OSAS was based on the standard polysomnography system. Obstructive apnea was defined as a drop in airflow to ≤ 90% of baseline for ≥ 10s as recorded with the oronasal sensor. Hypopnea was defined as a drop in airflow ≥ 30% from baseline as recorded with the nasal cannula for ≥ 10 s accompanied by ≥ 3% oxygen desaturation or arousal. PSG parameters were measured by standard PSG System. Clinical data collection included the AHI, oxygen desaturation index (ODI), minimal arterial oxygen saturation (MiniSaO2), and mean O2 saturation (SaO2).
2.4. Cardiopulmonary Exercise Test (CPET)
A gas analyzer is the principal equipment for CPET. A breath-by-breath gas analyzer is necessary for a clinical setting. Additionally, a cycle ergometer or treadmill ergometer, as an exercise load device, and an electrocardiograph are necessary. A cycle ergometer is required to produce a sufficiently weak load because the exercise ability of these patients is very low. The gas analyzer measures the oxygen and carbon dioxide content in a gas. Using inspired and expired gas, oxygen uptake (VO2) and carbon dioxide output (VCO2) are calculated. The gas analyzer also measures tidal volume (TV) and respiratory rate (RR). From these measurements, minute ventilation (VE) is calculated. Using VO2, VCO2, VE, heart rate (HR), VE/kg, VO2/kg, and VCO2/kg are calculated. A breath-by-breath gas analyzer also measures the partial pressure of end-tidal oxygen and carbon dioxide (PETO2 and PETCO2). The testing starts with pulmonary function tests; the lab staff place monitors on the patient to watch their heart and breathing during exercise. Patients have EKG leads (wires attached to stickers) on their chest. A blood pressure cuff is placed on the upper arm. A pulse oximeter (measures the saturation of oxygen) is worn on the finger, and a mouthpiece or a mask (measures the oxygen and carbon dioxide that flow in and out) is worn during testing. Patients will choose a treadmill or stationary bike for exercise. The exercise is continued until the patient is no longer able to keep exercising. During the test, data about heart and lung responses to exercise is collected.
2.5. Statistical Analysis
The data is presented as mean ± standard deviation (SD), or median and interquartile ranges. Categorical variables are presented as frequencies and percentages. The predictive validity and optimal cut-off value were estimated using the receiver operating characteristic (ROC) curve. ANOVA analyses were carried out to evaluate the differences between the three groups. Data was analyzed using SPSS 18.0 software. The predictive validity and optimal cut-off value were estimated using the receiver operating characteristic (ROC) curve. A P-value of < 0.05 was considered statistically significant.
3. Results
3.1. Baseline of 68 Subjects
A total of 68 patients were enrolled in the final analysis. Demographic and clinical characteristics are presented in Table 1. In these cases, 68 subjects were diagnosed with OSAS. 20 patients, with an AHI < 15, were classified as the OSAS negative/mild group, 24 patients were in the moderate OSAS group (15 ≤ AHI < 30), and 24 patients were in the severe OSAS group (AHI ≥ 30). The three groups had no obvious differences in their clinical baseline data, demographic characteristics, and clinical characteristics. According to the results, we can see that all patients had an abnormal BMI, which should be less than 25.
Table 1. Demographic and clinical characteristics of the study group.
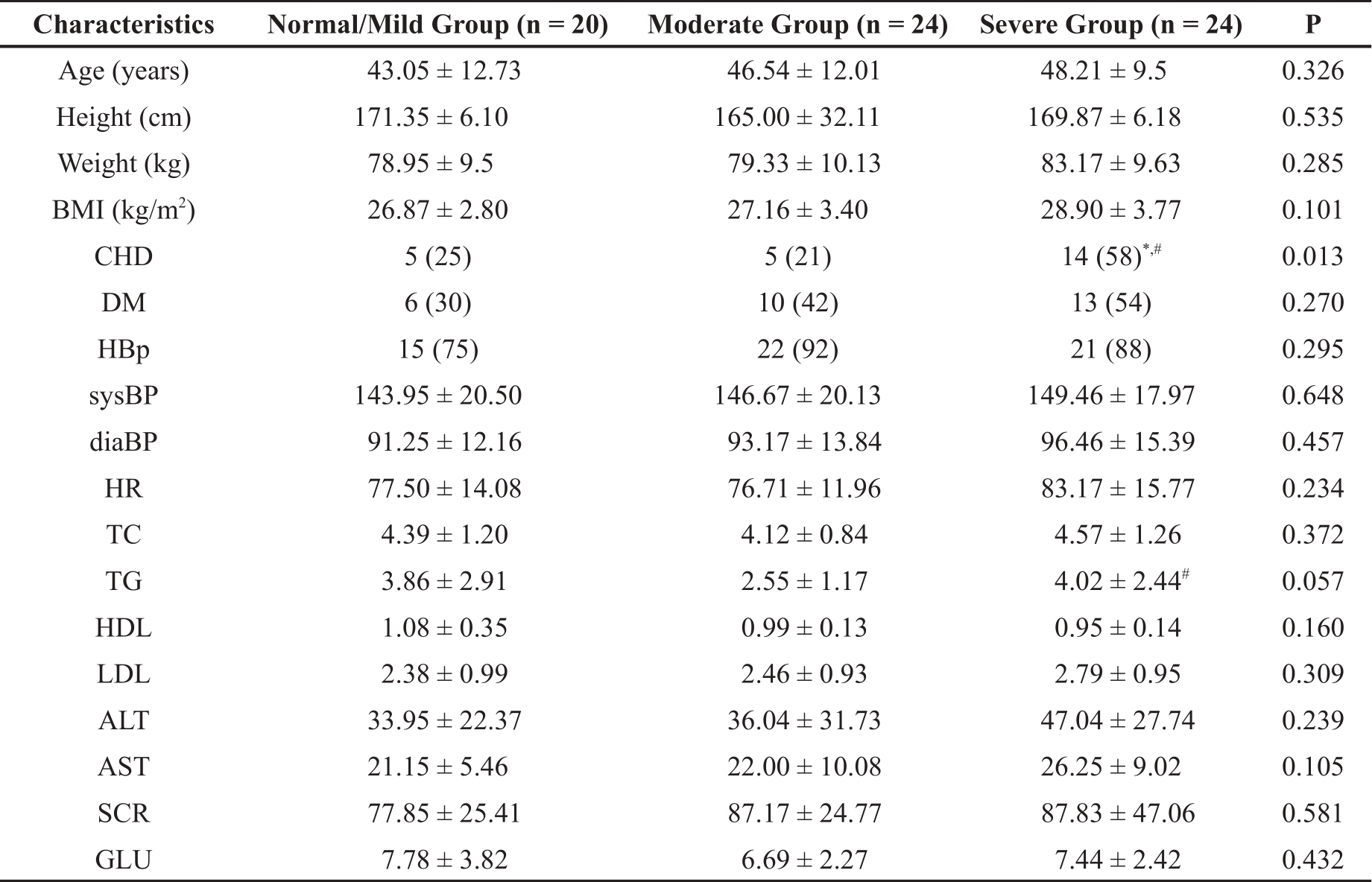
BMI: body mass index, CHD: coronary heart disease, TC: Total cholesterol, TG: triglyceride, ALT: Alanine transaminase, AST: aspartate transaminase, SCR: Serum creatinine, GLU: Glucose; * Represents a significant difference from normal/mild group; # Represents a significant difference from the moderate group.
3.2. Polysomnography (PSG) Parameters
The PSG results are shown in Table 2. The PSG data of ODI in the patients with moderate or negative/mild OSAS was significantly lower than patients with severe OSAS. MiniSaO2 and SaO2 levels in the severe OSAS group were significantly lower compared to the OSAS negative/mild group and moderate OSAS groups (P < 0.05; Table 2). We can see that blood oxygen saturation decreased with the aggravation of respiratory limitation.
Table 2. Comparison of PSG data in three groups.

AHI: apnea-hypopnea index, ODI: oxygen desaturation index, MiniSaO2: minimum percentage oxyhemoglobin saturation, meanSaO2: mean percentage oxyhemoglobin saturation, LAT: Longest apnea time; * Represents a significant difference from normal/mild group; # Represents a significant difference from the moderate group.
3.3. CPET Parameters
The CPET parameters of the three groups are shown in Table 3. The index of VO2 peak, VE start, VE peak, VO2/kg peak, VE/kg start, and VE/kg in the patients of the severe OSAS group was significantly lower than that of the moderate, and the OSAS negative/mild group. Finally, the logistic regression analysis results for the parameters of CPET among the three groups are shown in Table 4. We found that there is a relatively strong correlation between AHI index and the value of VO2 peak (r = 0.249, P = 0.04).
Table 3. Comparison of CPET parameters among the three groups.
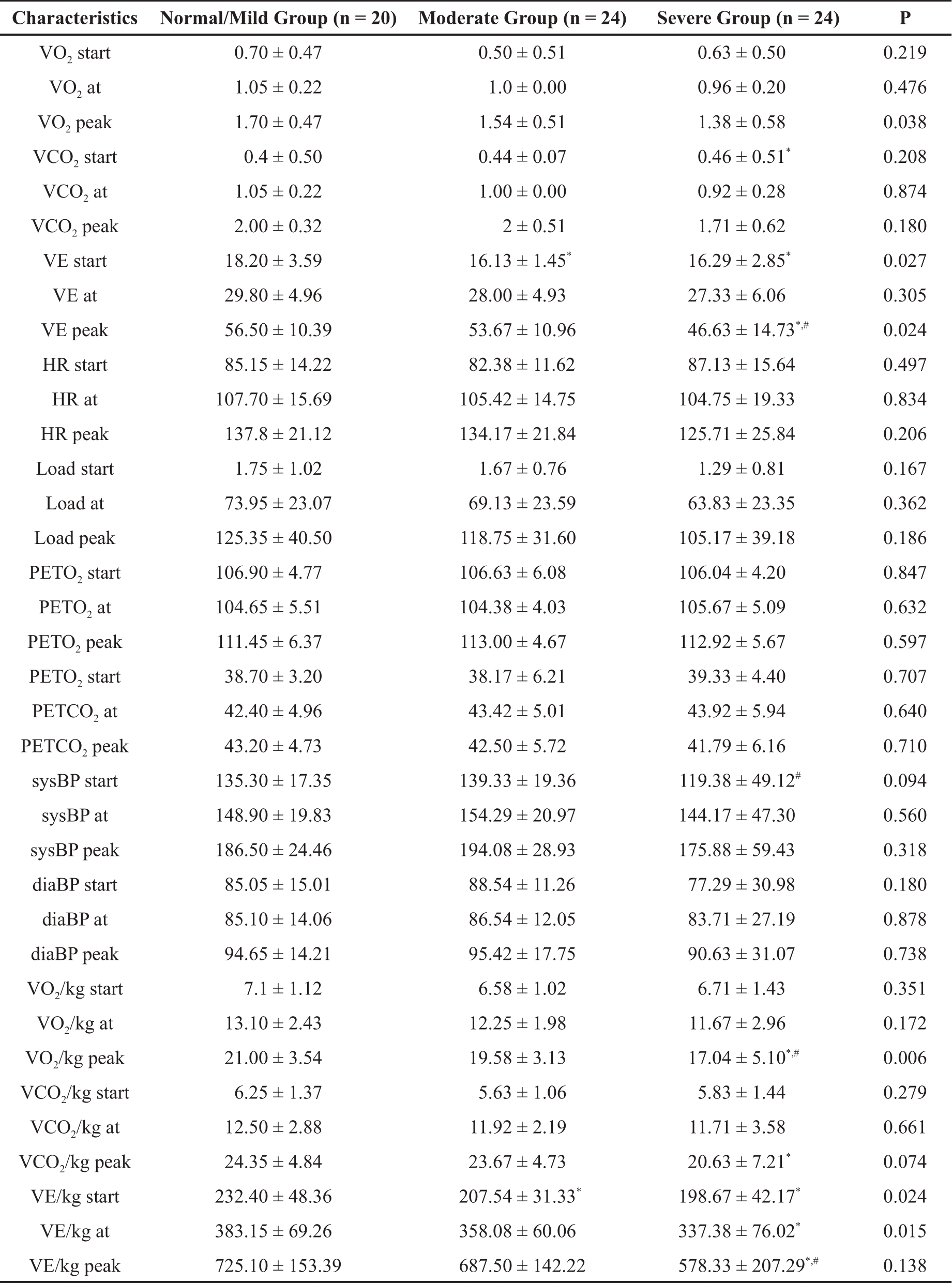
* Represents a significant difference from normal/mild group; # Represents a significant difference from the moderate group.
Table 4. Correlation of AHI with CPET data.
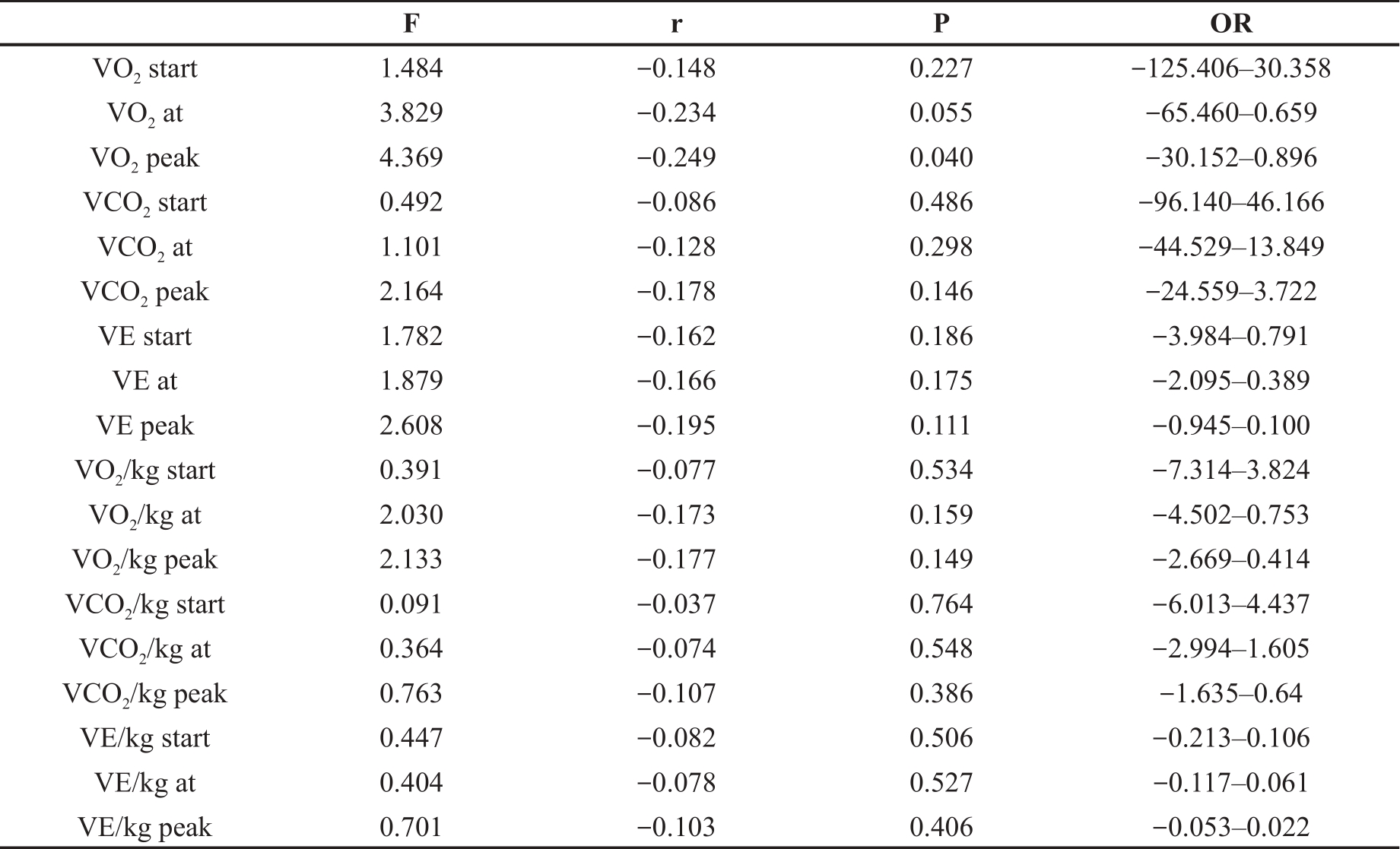
VE: minute ventilation; start: the start of the exercise; at: during the exercise; peak: at peak exercise. * Represents a significant difference from normal/mild group; # Represents a significant difference from the moderate group.
VE: minute ventilation; sysBP: systolic blood pressure; diaBP: diastolic blood pressure; start: the start of the exercise; at: during the exercise; peak: at peak exercise; PETCO2: end tidal carbon dioxide; PETO2: end tidal oxygen; P-values for comparisons of variables among three groups were calculated using ANOVA for continuous data and chi-squared tests for categorical data.
3.4. Association of AHI and CPET Parameters
In the previous study, we found a correlation between the AHI index and the value of the VO2 peak. The severity of OSAS improved with the increase in the VO2 peak (Figure 1). Previous research revealed that the index of CPET (VO2 peak, VE start, VE peak, VO2/kg peak, VE/kg start, and VE/kg) was associated with the severity of OSAS in patients, and the CPET index changed gradually as the severity of OSAS increased. Then we hypothesize that the CPET data can be used to predict the severity of OSAS.
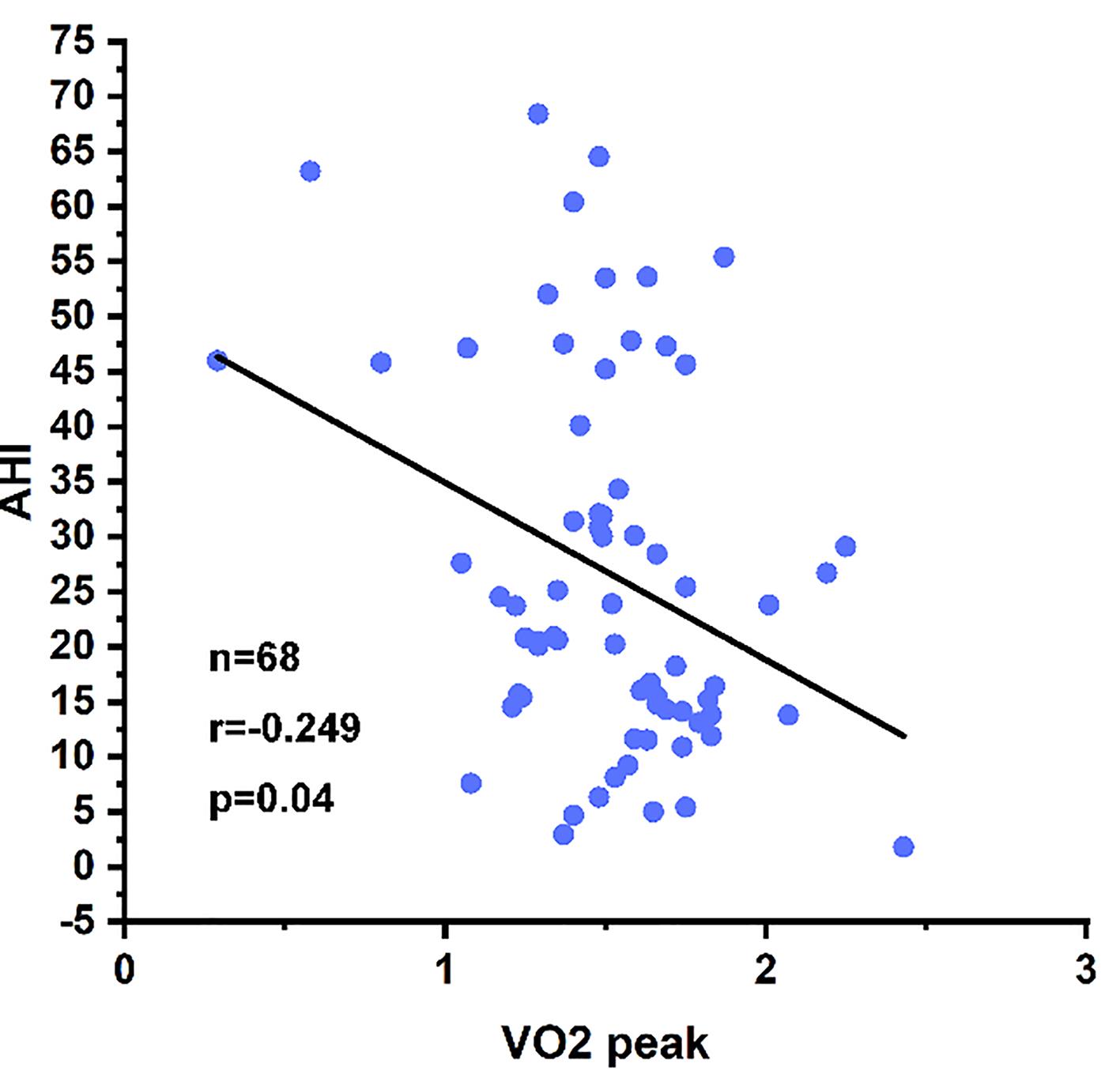
Figure 1. Scatter plot showing the relationship between apnea-hypopnea index (AHI) and VO2 peak.
3.5. ROC Analysis for the Predicted Efficiency Detection
Table 5 and Table 6 summarize the details of ROC analysis for each measured strain parameter, including operational cutoff values with corresponding sensitivity and specificity, AUCs, and p-values. In the VO2 peak and VO2/kg peak predictive group, ROC analysis showed lower AUCs (AUC = 0.321/0.313) and lower sensitivity/specificity (58.3%/25% and 54.2%/20%) in the detection of OSAS patients (AHI = 15). In the BMI predictive group, ROC analysis showed higher AUCs (AUC = 0.605) and sensitivity/specificity (60.4%/65%) in the detection of OSAS patients (AHI = 15), but the P-value was greater than 0.05 (P = 0.176), thus the predictive power was doubtful. Nevertheless, the predictive power of the CPET index (VO2 peak and VO2/kg peak) combined with the BMI index of patients, respectively, together with the detection of patient AHI (AHI = 15) was significantly improved. These groups had similar AUCs (0.708, 0.679, 0.835), but different sensitivity/specificity (56.3%/80%, 62.5%/70%, 64.6%/70%), and the P-value was less than 0.05. Therefore, it had significant predictive value.
Table 5. Receiver operating characteristic analysis of CPET data for the detection of patients with OSAS patients (AHI = 30).

Table 6. Receiver operating characteristic analysis of CPET data for the detection of patients with OSAS patients (AHI = 15).

Receiver operating characteristic plots of AUCs and P-values in Figure 2 illustrate the predictive power of the CPET index solely and the CPET index combined with the BMI index of patients in the detection of patient’s AHI. When CPET index (VO2 peak and VO2/kg) recombined with the BMI index of patients, respectively or together, the predictive power was significantly increased. Nevertheless, considering that the individual weight difference will have a greater impact on oxygen consumption, we put the parameters after weight correction into the total prediction model. Receiver operating characteristic plots of AUCs and P-values in Figure 2 illustrate the predictive power of the CPET index solely and the CPET index combined with the BMI index of patients in the detection of patient AHI.

Figure 2. Receiver operating characteristic analysis for the detection of AHI = 15 and 30 in the groups of BMI, VO2/kg peak, and BMI + VO2/kg peak. AUC = area under curve; BMI = body mass index.
4. Discussion
OSAS is an underdiagnosed chronic disease that is common in adults, and it is becoming a significant social problem. OSAS is caused by a variety of pathophysiological factors, including airflow limitation caused by the structural and functional changes of the upper respiratory tract, and the weakening of neuromuscular coordination [12]. Many studies have shown that obesity is an essential independent factor in OSAS, and is also linked to reduction in sleep quality and quantity. Weight loss has been shown to be an effective treatment for improving OSAS [13]. At the same time, OSAS patients have an increased risk of cardiovascular events and various metabolic diseases. Patients with OSAS often show nocturnal intermittent hypotension and apnea. Long-term intermittent hypotension can stimulate peripheral chemical receptors and enhance sympathetic nerve activity, resulting in the release of renin, angiotensin and aldosterone. This results in long-term contraction of peripheral blood vessels and increases the risk of cardiovascular diseases, such as hypertension [14]. At the same time, intermittent hypoxia can damage the function of mitochondria; activate the oxidative stress system; promote the release of proinflammatory factors; and aggravate vascular endothelial injury. Thus, the risk of cardiovascular events, including hypertension and atherosclerosis, is increased in OSAS patients [15,16]. CPAP as a treatment for patients with OSAS is not tolerated by all patients. Meanwhile, pharmacological intervention also has been proposed as an alternative to CPAP in some groups of patients. But there is currently no pharmacological agent approved for the treatment of OSAS. The mechanisms by which drugs might improve OSAS include: a reduction in the proportion of rapid eye movement sleep, an increase in ventilatory drive or an increase in upper airway muscle tone during sleep. Acetazolamide was shown to reduce the number of respiratory events but it cannot improve sleep quality or reduce the subjective impression of sleepiness in the day. Protriptyline has been the best studied drug, in two out of three studies participants reported a decrease in daytime somnolence [17]. PSG, also known as a sleep study, is an integral component of many sleep evaluations. It can confirm the sleep condition by measuring the AHI, and the lowest blood oxygen saturation. The AHI was measured to reflect the number of apnea times during sleep at night and the lowest oxygen saturation represented the most severe hypoxia event. There’s no doubt that PSG was considered the gold standard for diagnosis of and managing sleep-related breathing disorders, including OSAS, due to the fact that it can be used to analyze the breathing, and cardiac disturbances during sleep simultaneously [18]. However, the method also has some limitations. Many sleep disorders have night-to-night variability; thus, a single night measure may not truly reflect an individual’s normal sleep pattern. The PSG results are also affected by many factors, including the psychological factors and sleeping posture. At the same time, the body has a strong reserve function, and early blood oxygen saturation may not fluctuate greatly, which limits the use of sleep breathing monitoring and affects the accuracy of the test results [19]. Meanwhile, it is a cumbersome and expensive test. Patients are required to sleep overnight in the sleep laboratory. Many instruments are connected to the patient during PSG, including electroencephalography (EEG), electrooculography leads, a nasal pressure transducer, oronasal thermistor, and a pulse oximeter probe. All of these will influence the comfort level of subjects, which can also affect the results of the PSG [20]. Therefore, there is a need to find a more convenient way to diagnose OSAS.
The CPET is used to assess the exercise tolerance of subjects and the causes of exercise limitation through abnormal physiological indicators that occur in patients during exercise and is widely used to assess the cardiopulmonary function of subjects and for exercise instruction [21]. When combined with exercise testing, adjunctive imaging provides greater diagnostic accuracy, additional information about cardiac structure and function, and additional prognostic information. The person expressing the symptoms of unexplained shortness of breath, chest pain, and leg fatigue during exercise are suitable to get a CPET. Currently, CPET is used to determine the treatment prognosis of heart failure, COPD, coronary artery disease, and other cardiopulmonary diseases [22]. In recent years, increasing studies have been investigating the relationship between CPET and OSAS. The CPET is composed of several parts, including a gas analyzer, a cycle ergometer (an exercise load device), and an electrocardiograph. The CPET is much more convenient and economical compared to PSG. In previous research, patients with OSAS presented a lower VO2 peak and VO2/kg peak. The ΔPETCO2 max peak (the difference in PETCO2 between the maximum value reached during exercise and peak exercise) was used to suggest OSAS in patients with obesity [23]. Our previous studies have found a better correlation between AHI index and VO2 peak with CPET index in OSAS patients (r = 0.249, P = 0.04); also, obesity is an essential factor in the development of OSAS and that the majority of OSAS patients are obese. Hence, we hypothesized whether these indicators could be used to predict the severity of sleep apnea in patients with OSAS. A subject operating characteristic curve (ROC) analysis was performed to assess its efficacy in predicting the AHI of patients with OSAS. We found that the receiver operating characteristic analysis for the detection of AHI = 15 or AHI = 30 in the group of BMI, VO2 peak, and VO2/kg peak was not significant, and the AUC of VO2 group and VO2 peak group was less than 0.7. Furthermore, the P-value of BMI group was more than 0.05, which was considered not clinically significant. Because the predictive power of a single factor was not significant, we combined the patient's BMI and CPET index to predict the severity of OSAS. We found that the receiver operating characteristic analysis for the detection of AHI = 15 or AHI = 30 in the groups of BMI + VO2 peak, BMI + VO2/kg peak, and BMI + VO2 peak + VO2/kg peak were interesting, the ROC > 0.7 and the P < 0.05, which was considered clinically significant. Meanwhile, considering the different individual weights, we put the parameters after weight correction into the total prediction model. Altogether, this may be a new way to diagnose the severity of OSAS.
Nevertheless, as an exercise test method, CPET also has its limitations. Patients with poor muscular and skeletal conditions are unable to complete the test on a treadmill or stationary power bicycle; patients with severe hypertension and other acute and chronic diseases are not suitable for this exercise test; patients with impaired consciousness are unable to cooperate with the exercise test; and patients who are not cooperative enough and are not willing to do their best to achieve maximum exercise intensity. Fatigue, dyspnea, and pain during exercise limit the applicability of cardiorespiratory exercise testing and affect the accuracy of the test results [23,24]. Combining the cardiopulmonary exercise test with BMI to predict the severity of sleep apnea in OSAS patients was more comprehensive; it can be used as an indicator for early monitoring, guiding the subsequent treatment, as well as assessing the treatment effect, which are important for preventing serious complications and improving prognosis. In summary, we suggest BMI combined with CPET as an objective and easily reproducible predictor of OSAS. However, there are still some undiscovered reasons as to why the conclusion was not clinically significant when the female patients were included in the research. Epidemiologic studies have shown that OSAS is more prevalent in men than in women (4% vs 2%) [20]. Meanwhile, compared with female patients with OSAS, male patients were heavier, had a higher BMI, had higher systolic blood pressure, had shorter duration of slow wave sleep, had more micro-arousal events, worse AHI, and had more complex sleep apnea events. Although the ways to diagnose the OSAS patients were clinically significant, the definite relationship between BMI and CPET was not clear, and the specific mechanism of prediction of AHI score in OSAS patients needs further study. We can better understand the pathogeny of OSAS in patients through CPET, so as to better adjust the drug treatment plan. The drug treatment plan can be adjusted according to the patient 's own limitation.
5. Conclusion
Our study demonstrates that CPET combined with BMI can be used to predict the severity of OSAS in male patients. Our results show that, compared with the individual CPET parameters, when the BMI of patients was included in the prediction model, the prediction efficiency is significantly improved. Our study provided a new method to predict if the patients are in the early stage of OSAS. Through CPET, we can better provide drug treatment options.
Author Contributions: Conceptualization, Z.H. and C.Z.; methodology, Z.H.C.Z.; formal analysis, W.J.; investigation, Z.H.; resources, S.Z.; data curation, L.J.; writing—original draft preparation, W.J.; writing—review and editing, W.J.; visualization, Z.H.; supervision, Z.H.; project administration, Z.H.; funding acquisition, Z.H. All authors have read and agreed to the published version of the manuscript.
Funding: The project was supported by a grant from the National Natural Science Foundation of China (No. 81873535) and the Natural Science Foundation of Hubei Province (No. 2020CFB573).
Data Availability Statement: Not applicable.
Conflicts of Interest: The authors declare no conflict of interest.
References
- Lee J.J.; Sundar K.M. Evaluation and Management of Adults with Obstructive Sleep Apnea Syndrome. Lung, 2021, 199(2). doi: 10.1007/s00408-021-00426-w. DOI: https://doi.org/10.1007/s00408-021-00426-w
- Lévy P.; Kohler M.; McNicholas W.T.; et al. Obstructive sleep apnoea syndrome. Nat. Rev. Dis. Primers., 2015, 1: 15015. doi: 10.1038/nrdp.2015.15. DOI: https://doi.org/10.1038/nrdp.2015.15
- Kuvat N.; Tanriverdi H.; Armutcu F. The relationship between obstructive sleep apnea syndrome and obesity: A new perspective on the pathogenesis in terms of organ crosstalk. Clin. Respir. J., 2020, 14(7): 595-604. doi: 10.1111/crj.13175. DOI: https://doi.org/10.1111/crj.13175
- Scrutinio D.; Guida P.; Aliani M.; et al. Age and comorbidities are crucial predictors of mortality in severe obstructive sleep apnoea syndrome. Eur. J. Intern. Med., 2021, 90: 71-76. doi: 10.1016/j.ejim.2021.04.018. DOI: https://doi.org/10.1016/j.ejim.2021.04.018
- Adir Y.; Humbert M.; Chaouat A. Sleep-related breathing disorders and pulmonary hypertension. Eur. Respir. J. 2021 Jan 5;57(1):2002258. DOI: https://doi.org/10.1183/13993003.02258-2020
- Guimarães K.C.; Drager L.F.; Genta P.R.; et al. Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. Am. J. Respir. Crit. Care Med. 2009;179(10):962-966. DOI: https://doi.org/10.1164/rccm.200806-981OC
- Tanriover C.; Ucku D.; Akyol M.;e alt., Potential Use of SGLT-2 Inhibitors in Obstructive Sleep Apnea: A new treatment on the horizon. Sleep & Breathing, 2023. 27(1): p. 77-89. DOI: https://doi.org/10.1007/s11325-022-02606-1
- Engstrøm M.; Rugland E.; Heier M.S. Polysomnography (PSG) for studying sleep disorders. Tidsskr. Nor. Laegeforen., 2013, 133(1): 58-62. doi: 10.4045/tidsskr.12.0172. DOI: https://doi.org/10.4045/tidsskr.12.0172
- Stavrou V.; Boutou A.K.; Vavougios G.D.; et al. The use of cardiopulmonary exercise testing in identifying the presence of obstructive sleep apnea syndrome in patients with compatible symptomatology. Respir. Physiol. Neurobiol., 2019, 262: 26-31. doi: 10.1016/j.resp.2019.01.010. DOI: https://doi.org/10.1016/j.resp.2019.01.010
- Guazzi M.; Bandera F.; Ozemek C.; et al. Cardiopulmonary Exercise Testing: What Is its Value? J. Am. Coll. Cardiol., 2017, 70(13): 1618-1636. doi: 10.1016/j.jacc.2017.08.012. DOI: https://doi.org/10.1016/j.jacc.2017.08.012
- Wagner J.; Knaier R.; Infanger D.; et al. Novel CPET Reference Values in Healthy Adults: Associations with Physical Activity. Med. Sci. Sports Exerc., 2021, 53(1): 26-37. doi: 10.1249/MSS.0000000000002454. DOI: https://doi.org/10.1249/MSS.0000000000002454
- Maspero C.; Giannini L.; Galbiati G.; et al. Obstructive sleep apnea syndrome: a literature review. Minerva Stomatol., 2015, 64(2).
- Xanthopoulos M.S.; Berkowitz R.I.; Tapia I.E. Effects of obesity therapies on sleep disorders. Metabolism, 2018, 84: 109-117. doi: 10.1016/j.metabol.2018.01.022. DOI: https://doi.org/10.1016/j.metabol.2018.01.022
- Borel A-L. Sleep Apnea and Sleep Habits: Relationships with Metabolic Syndrome. Nutrients, 2019, 11(11). doi: 10.3390/nu11112628. DOI: https://doi.org/10.3390/nu11112628
- Liu X.; Ma Y.; Ouyang R.; et al. The relationship between inflammation and neurocognitive dysfunction in obstructive sleep apnea syndrome. J. Neuroinflammation, 2020, 17(1): 229. doi: 10.1186/s12974-020-01905-2. DOI: https://doi.org/10.1186/s12974-020-01905-2
- Maniaci A.; Iannella G.; Cocuzza S.; et al. Oxidative Stress and Inflammation Biomarker Expression in Obstructive Sleep Apnea Patients. J. Clin. Med., 2021, 10(2). doi: 10.3390/jcm10020277. DOI: https://doi.org/10.3390/jcm10020277
- Smith I.; Lasserson T.J.; Wright J. Drug therapy for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006 Apr 19;(2):CD003002. DOI: https://doi.org/10.1002/14651858.CD003002.pub2
- Jafari B.; Mohsenin V.; Polysomnography. Clin. Chest Med., 2010, 31(2): 287-297. doi: 10.1016/j.ccm.2010.02.005. DOI: https://doi.org/10.1016/j.ccm.2010.02.005
- Markun L.C.; Sampat A. Clinician-Focused Overview and Developments in Polysomnography. Curr. Sleep Med. Rep., 2020, 6(4): 309-321. doi: 10.1007/s40675-020-00197-5. DOI: https://doi.org/10.1007/s40675-020-00197-5
- Corral J.; Sánchez-Quiroga M-Á.; Carmona-Bernal C.; et al. Conventional Polysomnography Is Not Necessary for the Management of Most Patients with Suspected Obstructive Sleep Apnea. Noninferiority, Randomized Controlled Trial. Am. J. Respir. Crit. Care Med., 2017, 196(9): 1181-1190. doi: 10.1164/rccm.201612-2497OC. DOI: https://doi.org/10.1164/rccm.201612-2497OC
- Herdy A.H.; Ritt L.E.F.; Stein R.;et al. Cardiopulmonary Exercise Test: Background, Applicability and Interpretation. Arq. Bras. Cardiol., 2016, 107(5): 467-81. doi: 10.5935/abc.20160171. DOI: https://doi.org/10.5935/abc.20160171
- Malhotra R.; Bakken K.; D'Elia E.; et al. Cardiopulmonary Exercise Testing in Heart Failure. JACC Heart Fail., 2016, 4(8): 607-616. doi: 10.1016/j.jchf.2016.03.022. DOI: https://doi.org/10.1016/j.jchf.2016.03.022
- Krol K.; Morgan M.A.; Khurana S. Pulmonary Function Testing and Cardiopulmonary Exercise Testing: An Overview. Med. Clin. North. Am., 2019, 103(3): 565-576. doi: 10.1016/j.mcna.2018.12.014. DOI: https://doi.org/10.1016/j.mcna.2018.12.014
- Shepertycky M.R.; Banno K.; Kryger M.H. Differences between men and women in the clinical presentation of patients diagnosed with obstructive sleep apnea syndrome. Sleep, 2005, 28(3): 309-314.


